





















Brain Puzzles
Dementia is a looming public health crisis. Are we any closer to understanding diseases of the brain? Max Cynader discusses the threat of Alzheimer’s, the promise of the latest research approaches, and his hopes for the recently opened Djavad Mowafaghian Centre for Brain Health.

It’s February, and on the fifth floor of the brand new Djavad Mowafaghian Centre for Brain Health the first few research scientists are settling in to their work stations, hooking up computers and monitors. “Come back in a month or two and there will be something like a hundred scientists here,” says Dr. Max Cynader, director of brain research at UBC. “I can’t wait till we’re up and running.”
The academic version of the Energizer bunny, Cynader is never still and talks a mile a minute. He is showing me through the striking and cleverly conceived building located on Westbrook Mall on UBC’s Vancouver campus, and is plainly delighted and proud. The $100‑million Centre for Brain Health manifests a collective vision that he has been leading for several years. It unites the often disjointed approaches of psychiatry and neurology, bringing together under one roof the clinical and research resources dedicated to the study, diagnosis, and treatment of the major brain‑related diseases: stroke, Parkinson’s, multiple sclerosis, traumatic brain injury, and Alzheimer’s.

Cynader has always been fascinated by the workings of the brain. “As a Jewish kid growing up in Montreal, I was told I could be an engineer, a lawyer, or doctor – choose one.” He giggles gleefully, which is how he reacts to most things. “As a 16‑year‑old student at McGill, I went into psychology. The reason is sort of ridiculous. My middle name is Sigmund – obviously I was destined to become a therapist! I could see the shingle outside my office: M. Sigmund Cynader!
“I soon discovered I wasn’t really interested in traditional psychology,” he continues, ducking down a light‑filled staircase to some wet labs on the fourth floor. “As an undergrad I had the good fortune to be taught by the legendary neuropsychologist D. O. Hebb. Neuropsychology teaches you that the brain ultimately determines your behaviour – how you’re going to think and act. I wanted to understand how neurons talk to each other, and what happens when this or that part of the brain was lost.”
By the time he went off to MIT in Boston to do his PhD (his thesis was on vision and brain development), he was permanently smitten. “I’ve been doing brain research for 50 years and I’ve never wavered, never lost interest. It was fascinating then, and we’re seeing ever more interest in diseases of the brain. The field keeps blossoming. It’s never been more fun.”
It’s never been more relevant, either. By 2020, brain disease is projected to overtake heart disease and cancer as the leading cause of death and disability in Canada. Dementia in its various forms consumes much of the $30 billion we spend annually treating brain dysfunction. Alzheimer’s, Cynader points out as we pass the Alzheimer’s clinic, is far and away the most prevalent expression of dementia.
At the moment, something like 750,000 Canadians are afflicted, a number expected to double within a decade. The number of dollars we spend each year caring for people with dementia is also ballooning. In the media, Alzheimer’s is often described in apocalyptic terms – an approaching catastrophe that, as populations age, threatens to bankrupt the world’s health‑care systems.
Is this the sort of tabloid hyperbole that can convince you, say, that killer bees will soon be on our doorstep? Is there really a looming crisis? “It’s a crisis right now,” says Cynader, whose academic honours, publications, and patents, if listed here, would fill the space for this article. “Ask me in five years and it will be a bigger crisis. Ask me in 10 and the word ‘catastrophe’ won’t be inaccurate at all. I have no idea how countries like China and the United States are going to deal with this. Or Canada, for that matter.”
Dr. Bob Cheyne, incoming president of the UBC Medical Alumni, can attest to the urgency of the situation. After three decades of family practice in White Rock, BC, he’s seeing what he calls “a tsunami” of dementia cases. “Partly it’s because life expectancy has increased so much. When I started out, average life expectancy was about 72 years. Now it’s over 80. As the baby boomers hit old age, we can only see more of it.”
Like most people in their 60s, Cheyne has seen the devastation at close hand. His mother, who’s 92, was diagnosed with Alzheimer’s three years ago. “She’s still able to live at home in Vancouver thanks to round‑the‑clock care,” he says. “Fortunately, we can afford it, but of course not everyone can. I think we need to change our approach to elder care. In some cultures, it’s up to families to look after the older generation. I think we need to move in that direction, through education and public policy. We need to be giving tax breaks to families facing those challenges. I don’t know how else we’re going to address the tremendous costs of long‑term care.”
Cynader, too, has felt the sting of dementia. His mother, in the course of succumbing to brain cancer, suffered all the symptoms associated with Alzheimer’s. And his mother‑in‑law, who lives in Cincinnati, was diagnosed with the disease many years ago. Her dementia has exacted a brutal financial and emotional toll. “It’s a condition,” he says, “that can tear families apart.”
Alzheimer’s is often described in apocalyptic terms – an approaching catastrophe that, as populations age, threatens to bankrupt the world’s health-care systems.
What, exactly, is Alzheimer’s? Dr. Howard Feldman, director of the Clinic for Alzheimer’s Disease and Related Disorders at the Centre for Brain Health, explains that afflicted people develop a progressive loss of cognitive abilities associated with abnormal deposits of proteins in the brain. These deposits form amyloid plaques and tau tangles. Neurons lose their capacity to function effectively. They progressively degenerate and die while their networks of connections through the brain’s synapses fail. With damage to the hippocampus, memory is affected. As neurons die en masse, the brain noticeably shrinks.
Much of the research at the Centre for Brain Health is organized around three fundamental goals. The first is an improved understanding of the mechanisms that determine how and why particular brain cells die, and how this might be prevented. The second is the promotion of functional recovery – the re‑growing of connections between cells that have been lost due to disease or injury. The third is the development of methods that will enable earlier diagnosis.
Daunting as the public‑health numbers are, both Feldman and Cynader believe Alzheimer’s is underreported. “By the time a patient gets diagnosed,” Cynader explains, “he or she has typically had the disease for at least 10 years. Patients might be recorded as having died of pneumonia, when they were actually prone to such diseases because they’d had dementia for 20 years and been bedridden for the last five. Officially they died with Alzheimer’s, not of it.”
Most Alzheimer’s diagnoses are made when patients are in their 60s, although people with inherited forms can present much earlier. Cynader has a friend whose wife was diagnosed in her 30s – “heartbreaking,” he says. People with Down syndrome, too, are susceptible. They have an extra chromosome that produces amyloid and many will develop the plaques and tangles associated with Alzheimer’s disease. Although this doesn’t mean that all go on to develop Alzheimer’s, the overall incidence of the disease in people with Down syndrome has been estimated at three to five times that of the general population.*
Are we any closer to understanding brain‑related diseases, and Alzheimer’s in particular? Brain science has benefitted tremendously from the tech revolution, says Cynader, especially in the area of neuro‑imaging. “Historically, we’d observe the effects of accidents and trauma, then work back from there. That’s a bit like putting a bullet through your computer and seeing if and how it still works.”
Multiphoton microscopy – a hundred times more powerful than magnetic resonance imaging – lets scientists see right down to the atomic units of connectivity in the brain. “Your brain has about 100 billion neurons,” he explains. “Each neuron only connects with about 10,000 other neurons. Not so different from human society, really – there are 7 billion people, but only about 150 of them are your friends. You can think of a neuron as seeking answers to the same questions people ask: Who shall I talk to? Who can I talk to? Who will listen to me? The ones that don’t integrate into a network don’t survive.
“Today I can put you in a scanner and see what parts of the brain are working in different circumstances. Say you have a fear of spiders. We can show you a spider, then bring it closer and see what parts of your brain get active. We can observe the differences in brain activity when you think of your grandmother, versus your grandfather. Or when you listen to Mozart, versus Shostakovich. We can see what’s wired together, exactly which brain cells are talking to each other. Being able to see all this in real time was unthinkable even 20 years ago.”
Positron emission tomography – the PET scan – uses nuclear medicine imaging to produce three‑dimensional, colour depictions of the functional processes within the brain – “a huge advance,” says Cynader. “Confocal and multifocal microscopy lets us put brain cells in a culture dish and watch as they form connections, develop synapses.”
We can observe the differences in brain activity when you think of your grandmother, versus your grandfather. Or when you listen
to Mozart, versus Shostakovich
Another major advance has been the genome project. Humans, we’ve learned, have about 20,000 genes (a gene being a piece of DNA that will eventually make a protein). “Fewer than we thought,” says Cynader. “In fact, we only have about half as many genes as rice.” More laughter.
“Roughly two‑thirds of those 20,000 genes are used to either grow your brain, or to operate it. It takes more genetic horsepower to make the brain than to make everything else in the body combined. In other words, most of genetics is actually neuroscience. I joke with my geneticist colleagues: ‘Oh, by the way, you’re working for us now!’”
Technology is not the only thing that has evolved. Since the Brain Research Centre was established in 2000, its multi‑disciplinary approach has given scientists from diverse fields unprecedented opportunities to work together. The new Centre for Brain Health takes the philosophy even further. The juxtaposition of research and clinical facilities encourages patients to become, in effect, collaborators. It provides novel learning opportunities for the next generation of brain scientists. And it creates an integrated environment in which research outcomes can be translated more quickly into therapies and treatments.
Has all this progress given rise to hope for Alzheimer’s patients, present and future? In the quest to define the underlying mechanisms of the disease, and to develop new diagnostic markers and drug therapies, are we slowing the tsunami? I put those questions to Howard Feldman.
“The epidemiology literature indicates that the prevalence and incidence rates of Alzheimer’s are actually decreasing,” he says, “as they are with stroke. Perhaps people are paying more attention to the factors that promote well‑being than the last generation did. But that’s just a small offset against the greying of the population.”
Disease modelling suggests that if we can delay the onset of Alzheimer’s by five years, Feldman adds, we could cut the prevalence by 50 per cent. Delay it by one year and we’d cut it by 10 per cent. “Ten per cent may not sound like much, but it would make a huge public health difference.”
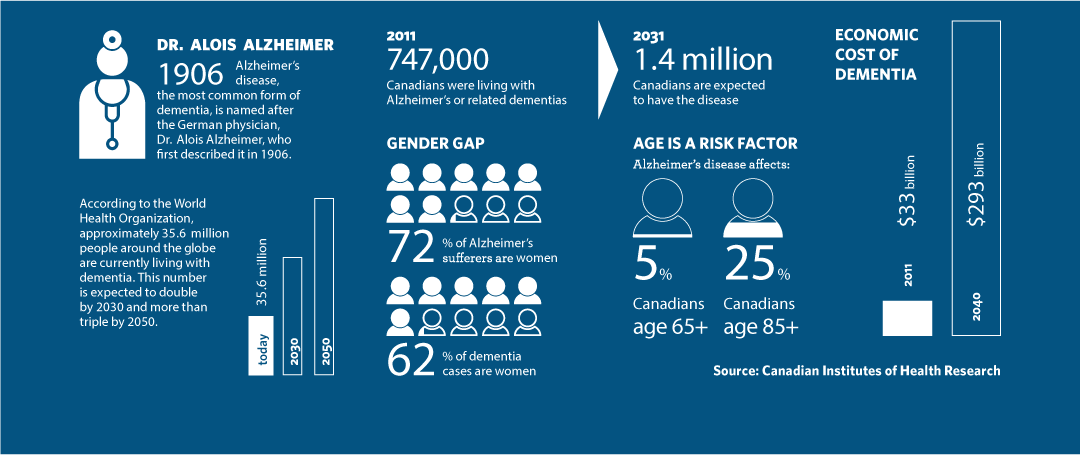
Alzheimer’s Facts
Dr Alois Alzheimer: Alzheimer’s disease, the most common form of dementia, is named after the German physician, Dr. Alois Alzheimer, who first described it in 1906.
According to the World Health Organization, approximately 35.6 million people around the globe are currently living with dementia. This number is expected to double by 2030 and more than triple by 2050.
In 2011, 747,000 Canadians were living with Alzheimer’s or related dementias. In 2031, 1.4 million Canadians are expected to have the disease.
Gender Gap: 72% of Alzheimer’s sufferers are women. 62% of dementia cases are women.
Age is a risk factor: Alzheimer’s disease affects: 5% Canadians age 65+ and 25% of Canadians age 85+.
Economic cost of dementia: In 2011, $33 billion. In 2040, $293 billion.
Source: Canadian Institutes of Health Research
Highlights from 60 Years of Brain Research at UBC
1956
From 1956, Drs. Patrick and Edith McGeer provided early leadership in Alzheimer’s research and received international recognition, attracting other high-calibre researchers to UBC over the following decades.
1991
Howard Feldman launched one of Canada’s most important clinical dementia research programs at UBC.
1998
Brain Research Centre established with Cynader as head.
2000
Two federal programs – the Canada Research Chairs program and the Canada Foundation for Innovation – allowed UBC to recruit more top brain researchers and develop world class research facilities. UBC becomes an important global hub for brain research in three key areas: neurodegenerative disorders, stroke and mental health and development.
2005
Dr. Weihong Song is an Alzheimer’s researcher who has identified important molecular targets for drug development. In 2005, he
fostered the development of a $15M Canada-China research collaboration between the Natural Science Foundation of China and
the Canadian Institutes of Health Research.
2006
Feldman and Ian MacKenzie discover the gene responsible for a common form of early-onset dementia. In 2011 MacKenzie discovers the same gene causes ALS, which causes the body’s muscles to rapidly weaken.
2011
Dr. Neil Cashman discovered a deformed protein that may lead to an eective therapy for ALS. A leading expert in protein-folding
diseases, Cashman has also developed a diagnostic test for early stage Alzheimer’s that is being evaluated by several pharmaceutical companies.
2014
The Djavad Mowafaghian Centre for Brain Health opens.
How do we get there? “We need to mobilize around a national plan that centres on prevention and care. Fourteen countries now have an overarching national plan, but Canada is not one of them. We need a system that’s flexible and full of good ideas, but we’re hamstrung by political considerations. Instead of putting a call outfor big ideas and bold thinking, we tend to be limited by considerations of governance and administration. A national plan needs to override health mandates being a provincial matter.”
It’s not just a public policy issue, of course. Individuals can modify their behaviour to lower their chances of developing dementia, or at least to delay its onset. How? Max Cynader offers this practical advice: “Stay active. Exercise regularly. Eat well – put lots of different colours on your plate – and don’t overeat. Though the brain weighs only about 1.5 kilograms, it requires 20 per cent of the blood supply. Anything that’s bad for the heart is bad for the brain. A drink or two of alcohol appears to be salutary, but 10 or 20 drinks are not.”
Though the brain weighs only about 1.5 kilograms, it requires 20 per cent of the blood supply. Anything that’s bad for the heart
is bad for the brain.
We’ve made our way through the patient care and assessment facilities on the second and first floors, and I’ve just been shown the subterranean room where brains are removed from cadavers. Here in the spacious lobby on the ground floor, beneath gigantic, stylized neurons on the huge walls of glass, our tour comes to an end.
Cynader, now 66, is stepping down as director in June. The centre is a reality at last, much of his time in recent years been devoted to fundraising and administration, and he’s eager to get back to his first love: research.
Taking my leave, slapping my pockets, I joke that lately I keep forgetting where I’ve left my keys.
“Not remembering where your keys are happens to everybody,” says Max Cynader. “If you can’t remember what they are” – laughter again – “it’s time to come back and see us.”
* This online issue of the magazine is adapted from the spring 2014 print edition, which inaccurately stated that most people with Down syndrome develop Alzheimer's in their 30s or 40s.
History and Highlights of Brain Health Research at UBC
The Djavad Mowafaghian Centre for Brain Health

The Djavad Mowafaghian Centre for Brain Health is Canada’s largest integrated brain centre. Powered by a dream team of clinicians, care providers and researchers, the DMCBH is a partnership between UBC and the Vancouver Coastal Health Research Institute and was named for its principal funder, Djavad Mowafaghian, who donated $15M as part of UBC’s start an evolution fundraising and alumni engagement campaign.






{kind=link}
{kind=link}